Editor’s Note: This the third part of an article series. The first part focused on running the trim and the second on wreckage and pilots' flying history.
The Interstate Aviation Committee (MAK-IAC) of the Russian Federation focused its accident analysis of the FlyDubai Flight 981 accident on four subjects: the crew’s conduct of the flight, the use of pitch trim, the use of the HUD during go-around, and the effect of somatogravic illusion.
Conduct of the flight: Analysis of the flight showed that the crew had shown a high level of training and proficiency, and the captain was the indisputable leader throughout the flight. At the point of initiating the second go-around, the captain began to make errors, take inappropriate actions and relinquish leadership. After his gear-up command, the captain did not give another command; he only uttered four brief phrases, including a noticeable exhalation of breath. His decision to go around conflicted with his intention to land, and this conflict caused him to “fall behind” the rapidly accelerating airplane.
When the first officer (FO) prompted “Flaps 15,” it was a deviation from the planned windshear escape maneuver, but the captain consented. The resulting low drag, along with the maximum power setting and low aircraft weight, caused the airplane to climb and accelerate rapidly, and the captain could not maintain the necessary 15-deg. nose-up pitch despite further prompting from the FO. When the captain initiated nose-down pitch trim, the flight went from an abnormal to an emergency situation. The stabilizer trim motor moved at twice the normal speed because the flaps were extended, and the captain’s continued forward pressure on the yoke resulted in a near-zero and negative G condition. This caused or exacerbated the captain’s spatial disorientation. He did not respond to the FO’s attempts to correct his actions and did not release the trim switch for 12 sec. The captain’s actions led to a rapid decrease of pitch (an average pitch rate of about 6 deg./sec.) and the aircraft’s transition from climb to descent with significant negative G. The G load decreased from -0.3 to -1.07 and remained at near zero or negative values thereafter.
At the time of the captain’s fatal actions, the flight had been airborne for 6 hr., including 2 hr. under intense workload. It was 4:42 a.m. on their circadian body clocks, the lowest point in the day for human ability to perform.
Use of pitch trim: By holding nose-down force on the control column while at the same time using the electric trim motors to change the angle of the stabilizer to a more nose-down position, the captain betrayed a lack of understanding of the 737 trim system. On the 737, as on virtually all modern commercial aircraft, the entire stabilizer moves when trim is applied. The elevator should be neutralized when trim is applied. The captain probably expected control force to be reduced as he trimmed, as would happen in a small training airplane that has a fixed stabilizer and a trim tab on the elevator. In fact, control force on the 737 is provided artificially by a feel and centering mechanism.
The Boeing flight crew training manual (FCTM) used by FlyDubai and most other airlines to train pilots contains a statement that pilots should not fly the airplane using stabilizer trim. However, a more-detailed explanation of how trimmable horizontal stabilizers work was not provided. When queried by investigators, Boeing officials stated that knowledge of trim forces is part of the basic airmanship needed to fly large transport airplanes, and this knowledge is a prerequisite to training on the 737. Boeing did, in fact, provide such information in Boeing Airliner magazines in 1959 and 1961 when moveable stabilizers were first introduced on the 707 and 720. Gradually, over time, understanding of the stabilizer was supposed to have become common knowledge.
Managers, pilots and instructors at FlyDubai told investigators they did not think the captain would have possessed a sufficient level of knowledge about trim forces on the aircraft to understand the need to neutralize the elevator when trimming. Investigators concluded that because he had only flown light aircraft before this model, he may never have been instructed on the proper way to trim the airplane.
The FO, who had flown the A320, an airplane with a trimmable horizontal stabilizer, was more likely to have understood the Boeing design. However, to trim opposite the captain’s nose-down force, he would have had to select override on the stab trim override switch, located at the aft end of the control pedestal. (As I recall, that guarded switch was a handy location to hold the cockpit trash bag but was never otherwise used.)
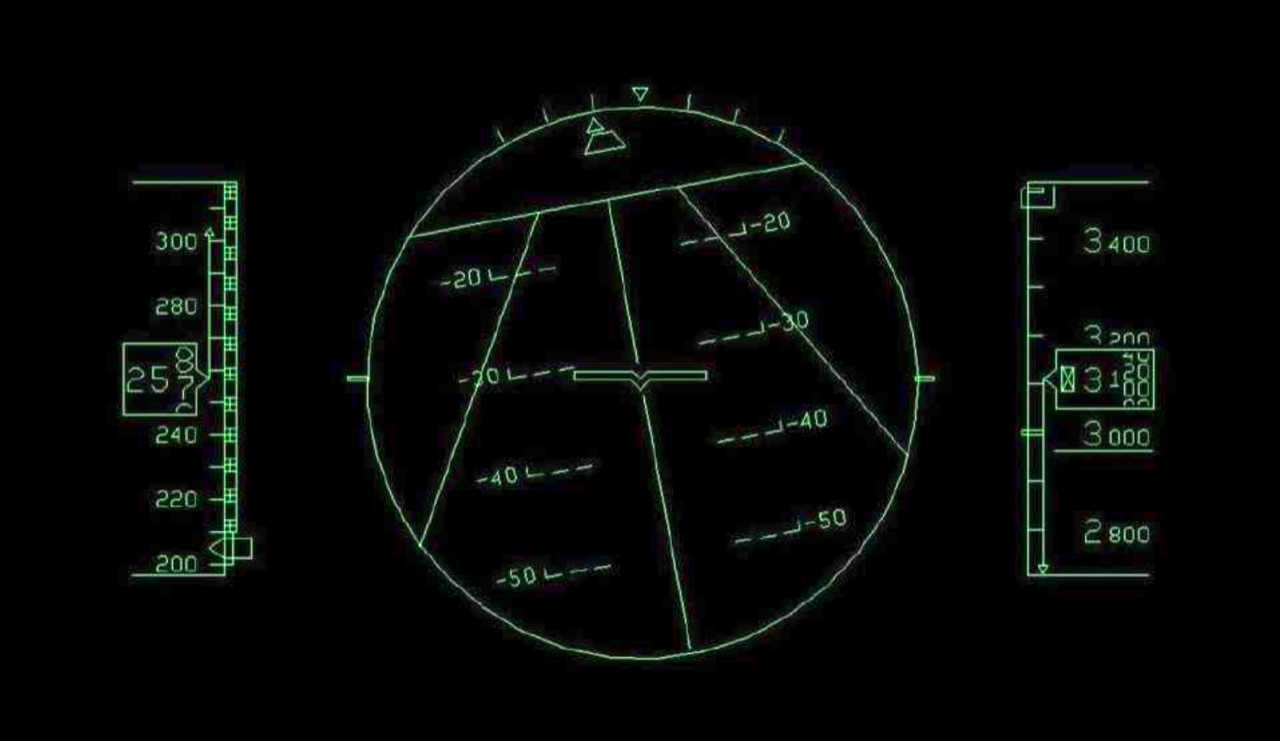
The HUD during go-around: At the request of investigators, the HUD manufacturer, Rockwell Collins, attempted to reconstruct the HUD display during the accident sequence. While the reconstruction was not “a complete and accurate reproduction of what the pilot was seeing,” it was nonetheless useful in understanding how the pilot may have lost spatial orientation.
While a main advantage of a HUD is the ability to observe the outside environment while being able to monitor primary flight parameters, under some circumstances, such as a night or IMC go-around or upset, seeing outside is not of value. If the HUD brightness is high or the pilot is overly focused on clouds and fog outside the airplane, he may become disoriented. A second concern is how well the pilot maintains his head posture relative to the HUD. In extreme conditions, such as turbulence or negative G, a portion of the HUD picture may go out of the pilot’s vision field. A third concern is whether the pilot is able to recognize the HUD depiction when in an extreme nose-down attitude.
The reconstructed HUD view when the airplane was 18-deg. nose low showed the horizon was still depicted, and a large, inverted V pointed in the direction the airplane should fly to recover from the extreme attitude. At 20-deg. nose low, the image simplified. The airplane symbol showed -20 deg., but two slanting lateral lines converging toward the top of the display appeared, and these lines could have been misinterpreted as a runway symbol. The same symbology was displayed when the airplane was 40-deg. nose low. It was doubtful that the pilot ever would have seen these HUD depictions during his simulator training.
While investigators could not unequivocally determine that the HUD contributed to the pilot’s disorientation, they felt there was enough concern that further testing of the HUD during different segments of flight should be done.
Somatogravic illusion: A significant longitudinal acceleration causes a vestibular illusion that the airplane is pitching up. In response, a pilot may push forward on the control column and, at low altitudes, fly into the ground. This somatogravic illusion has been causal or contributory in many accidents. In 2013, the French Bureau d’Enquêtes et d’Analyses (BEA) conducted a major study of go-around accidents that provided numerous examples of the phenomenon.
FlyDubai Flight 981 certainly experienced significant longitudinal acceleration during both its first and second go-around attempts. IAC investigators evaluated the accident flight using recorded data and a concept known as GIF (gravito-inertial force) to compare the actual flight path with an “illusory pitch” flight path. GIF is the longitudinal and vertical G effect on the pilot, and is computed by the formula GIF = arctg Nx/Ny, where Nx, Ny is longitudinal and vertical G.
Investigators plotted the GIF angle against actual pitch using FDR data and found four points during the last go-around where somatogravic illusion may have affected the captain. However, three of these points were only of short interval (4 sec., 4 sec. and 9 sec.). Most importantly, the go-arounds took place in visual flight conditions.
According to investigators, the illusion only takes place when there is no horizon or ground reference and monitoring of instruments is insufficient. The accident airplane did not pass the first scattered cloud deck on the second go-around until 14 sec. after initiating the maneuver, and never climbed above the broken cloud layer at 3,820 ft. QNH. The pitch-up illusion was strongest when the airplane was at negative G, but by that time stress and negative G had just as much effect on the pilot’s disorientation as somatogravic illusion. In addition, it did not appear that the FO ever experienced an illusion.
The investigative team concluded somatogravic pitch-up illusion “did not have crucial importance as far as the onset of the accident situation is concerned.”
The cause of the accident was judged to be “an incorrect aircraft configuration and crew piloting,” with a “subsequent loss of PIC’s situational awareness in nighttime in IMC.” There were 10 contributing factors, which broke down into six crew-related factors, two factors due to conditions and two procedural factors.
The crew-related contributing factors were:
*The captain’s lack of psychological readiness for the go-around.
*The captain’s loss of leadership and confusion.
*The crew’s uncoordinated actions during the go-around.
*The captain’s inability to maintain the required pitch.
*The captain’s insufficient knowledge of manual trim operation.
*The captain’s incapacitation and disorientation.
The contributing conditions were turbulence and windshear, and crew fatigue. The procedural factors were the lack of a required “go around” callout, and the lack of stated criteria for psychological incapacitation.
When a well-trained, well-qualified crew loses control of an airplane and experiences a catastrophic accident, trying to understand why it happened is a tough task. I think the IAC did a convincing job of showing that this accident was more than simply the result of somatogravic illusion. A go-around is one of the more difficult maneuvers pilots must perform. The longitudinal Gs that accompany the rapid acceleration of a high-thrust airplane cannot be duplicated in training, even in full-motion simulators. The first time a pilot experiences it may very well be on a revenue flight, and that may have been the case with the accident crew. Despite all their training, they weren’t prepared for this situation.
Chief among the IAC’s causal factors was the captain’s mismanagement of the pitch trim. It’s hard to imagine how a pilot could hold a trim switch for 12 sec. in any airplane without losing control. Given the amount of forward pressure the captain was exerting on the yoke (up to 50 lb.) and the tunneling of his attention that went with increasing mental and physical stress, it’s very likely he simply lost track of what his thumb was doing. That’s one reason that building a reflexive technique of trimming in short clicks is important. Even when you lose track of your thumb, you are not holding down the trim switch.
I would add one more cause to the IAC’s list: plan continuation bias. Professional pilots are almost universally confident and goal oriented. As a result, they are prone to try to complete every flight to its intended destination, even when doing so is unwise or even impossible. In retrospect, it is clear that the windshear conditions at Rostov-on-Don the night of the accident made landing there impossible. The FO said as much in the conversation he had with a flight attendant. He should have had that conversation with the captain, but he didn’t.
Pilots don’t like to hear the complaints from disappointed passengers and cranky dispatchers when they have to divert, but it goes with the territory. The ability to say no is a mark of a veteran pilot. The pilot has learned how to steel himself or herself from the critics, especially the biggest one—one’s self.

Related Content




