Editor's Note: The article describing the flight leading up to the accident can be found here.
A fatal flight on the night of March 19, 2016, a tired and frustrated pilot lost control of the Boeing 737-800 he was flying while attempting his second go-around in turbulent, gusty conditions. The aircraft impacted the ground at a speed of about 340 kt., with 50-deg. nose-down pitch and in a left bank of 60 deg.
The Interstate Aviation Committee (MAK-IAC) of the Russian Federation conducted the investigation, assisted by representatives from the U.S., France and the United Arab Emirates. The IAC also obtained assistance from other internal and external groups, including pilots and instructors from several Russian airlines. The Spanish investigative authority (CIAIAC) translated and transcribed the portion of the CVR that was in Spanish. The investigation, which took place over a period of two years and eight months, was completed in November 2019.
The aircraft was a Boeing 737-8KN manufactured in 2011. It had 21,257 hr. of flight time and 9,421 landings. The CFM56 engines were installed on the aircraft in 2014 and were midway through their service life of 20,000 cycles. No maintenance issues or discrepancies were found. Examination of weight and balance records showed the airplane was properly loaded and had sufficient fuel for the flight.
The aircraft’s fuselage, wings, flight controls, stabilizer and landing gear were disintegrated into many fragmentary elements. The impact formed a crater 30 to 40 ft. in length and about 5 ft. deep. The FDR was found; the quality of the recording was good and the duration was over 26 hr. The CVR was also found and had a good quality recording for just over 2 hr.
Although neither the ATC communications nor the data recorders indicated any mechanical malfunctions, the IAC conducted a very thorough investigation of the stabilizer jackscrew, the elevator power control units (PCUs), and the condition of the electric stab motor. Their extra diligence may have been due in part to their experience investigating the crash of a Boeing 737-500 in Kazan, Russia, in 2013. In that accident, they found the cause was management and oversight deficiencies, resulting in the crew not being qualified. Similar to the FlyDubai accident, the flight experienced an excessive nose-up attitude during a go-around, followed by a crash onto the approach end of the runway. No mechanical faults were found, but one member of the commission disagreed with the IAC’s findings and asserted that they had not adequately considered a possible malfunction of the elevator controls. The dispute resulted in a temporary grounding of 737s in Russia.
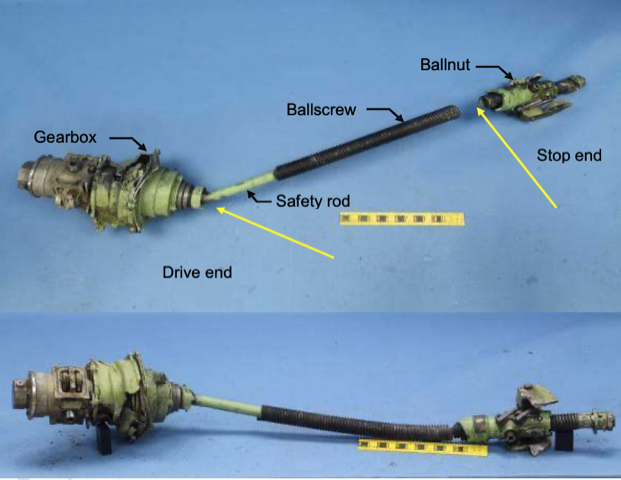
Part of the stabilizer trim actuator was found, but it was damaged and deformed. An examination of the stabilizer jackscrew showed it was consistent with FDR data, which showed no malfunction. The elevator power control units and the electric stab trim motor were also examined. The IAC went so far as to have the manufacturer of the elevator PCUs, Parker Aerospace, do a computed tomography (CT) examination of them and had the U.S. NTSB analyze the results. No faults were found. Similarly, the electric stab motor was tested by the manufacturer, Eaton, in the U.S. under the supervision of the NTSB, and no faults were found.
Working with Boeing, investigators conducted an engineering simulation of the last 90 sec. of the flight. FDR data was confirmed and data such as angle of attack, sideslip, TAS and wind were calculated. The simulation showed that icing was not a factor and that the flight could have pulled out of the final dive if a maximum pull of 125 lb. had been made no later than when the FO called out “Pull it, pull it!” Investigators also reconstructed an approximation of the HUD presentation the captain would have seen.
In reviewing previous go-around and mis-trim accidents, investigators highlighted the crash of an Ilyushin IL-86 in Moscow in 2002. Just after takeoff, one of the pilots pressed and held the stab trim switch to the nose-up position for 34 sec., resulting in the stabilizer going to its full airplane nose-up position of 12 deg. The airplane stalled and crashed, resulting in 12 fatalities and two injuries. Interestingly, the trim switch was held for 15 sec. after the stabilizer had reached its maximum position.
The FlyDubai accident captain had been employed at the company for 3.5 years, following stints as FO at the Malaysian Airlines system, XL Airways (Great Britain) and Helios Airways (Cyprus). He was 37 years old, a native of Cyprus, and had upgraded to captain at FlyDubai in January 2015, 14 months before the accident. Most of his flight experience was on various models of the Boeing 737 (4,682 hr. out of 5,965 total), and he had been busy, flying more than 45 hr. in the last 14 days and 843 hr. in the previous year. He had a valid Class 1 medical certificate and was rated at the highest level of English language proficiency (level 6 — expert). His training records were current and revealed no deficiencies. News reports after the accident stated he had complained to acquaintances about fatiguing working conditions and that he was planning to go to work for Ryanair, where he could expect to be based at home in Cyprus.
The FO, 36 years old, had been employed at FlyDubai since September 2014 and had accrued 1,100 hr. in the 737-800 since becoming qualified in the airplane. Like the captain, he had been busy, flying more than 55 hr. in the last 14 days and 784 hr. in the year before the accident. A native of Spain, he had flown for two Spanish regional carriers, Regional Geodata and Islas Airways, in the Cessna 421 and ATR 42/72, and had logged 5,767 total hours. He had 258 hr. of pilot in command time, and he was qualified on the Airbus A320. His English language proficiency was ICAO level 5 and his Class 1 medical certificate was valid and current.
Both pilots’ flight and duty times were within legal requirements, with the captain having flown 78 hr. and been on duty 136 hr. in the last 28 days, and the FO having flown 80 hr. and been on duty 139 hr. in the last 28 days. The captain had preflight rest of 15 hr. and the FO had 20 hr. Forensic analysis of the crew’s remains showed no evidence of drug or alcohol use by either pilot. The two pilots had never flown together before the accident flight, and the flight was the first to Rostov-on-Don for both.
FlyDubai had a fatigue management system (FMS) that encouraged confidential reporting by crewmembers. Over a seven-year period, the company had received 70 such reports and most resulted in crewmembers being removed from duty until they felt fit for flight operations.
The airline placed certain restrictions in their operations manual on flights to Rostov-on-Don Airport, Russia (URRR). Only the captain was permitted to fly the approach, landing and takeoff. There was a notice of the non-standard (2º40’) glideslope and a caution to confirm whether QNH or QFE altimeter settings were in use. There was also a note that turbulence and windshear on final were common problems.
FlyDubai’s 737 were all equipped with a HUD, installed on the captain’s side, and its use was mandatory throughout the entire flight. All pilots, including first officers, were trained in the simulator to use the HUD, both as pilot flying and as pilot monitoring. The initial HUD training included two all-engines operating go-arounds and two engine-out go-arounds.
During initial 737 training, all FlyDubai pilots performed 12 go-arounds, including some with various systems failures, from altitudes between 1,000 ft. and DH. The pilots practiced go-arounds due to low RVR, windshear, glideslope deviation, HUD failure and pilot incapacitation. During recurrent training, they performed three go-arounds, but none from higher altitudes than minimums or at low aircraft weight.
All company pilots received ground school training on predictive and actual windshear avoidance and recovery; simulator training on windshear was accomplished in initial and recurrent training. Both accident pilots had completed windshear training in 2015. They also had received training in manual stabilizer trim operation and upset recovery.
On the captain’s recurrent training and proficiency check in 2015, he failed to call out to set go-around thrust, and during the windshear training event he failed to press TOGA at the appropriate time, but he repeated the event satisfactorily. During the FO’s last two recurrent training events he had been debriefed on go-around execution. In one case, he was reminded that TOGA mode shows wings-level information, and on another he was reminded to call for go-around thrust. On a proficiency check one year prior to the accident, an instructor noted that the FO “needs to be quite a bit more assertive in what is needed from the captain. Tell him/her what you want done and do not wait for the captain to enquire with you or direct you in this regard. Need to be more decisive in taking actions when needed.”
Investigators noted that on their first approach, the accident crew incorrectly set a QFE altimeter setting of 990 hPa instead of the QNH value of 1,000 hPa. This 10-hPa difference corresponds almost exactly to URRR’s elevation of 280 ft. The mis-set altimeters resulted in the crew flying slightly higher than required on that approach. They corrected themselves on the second approach. The IAC noted in its report that although the error did not affect the outcome of the flight, the continued use of QFE altimetry in the Russian Federation “presents extra risks.”

Related Content




