Turkish Crew Starts Descent Too Late, Leading To Crash In Kyrgyzstan

On a dark and foggy night in 2017 the crew of a Turkish freighter came to grief in an autolanding that touched down off the airport in Kyrgyzstan, killing themselves, two relief crewmembers and 35 area residents.
After a three-year effort, Russian investigators have released their final report on the accident. In addition to a catalogue of human errors and missed opportunities to avoid the catastrophe, the report revealed a new twist on an automatic system involving the color green.
The all-cargo Turkish Airlines Boeing 747-412F flew a fully automated descent and executed a perfect autoland, including flare, but did so 3,050 ft. beyond the far end of the intended runway. The airplane touched down at 165 kt., smashed through an airport barrier wall and disintegrated along a 1,800-ft. path.
The Flight
Turkish Airlines Flight 6491 originated in Hong Kong (VHHH) and was destined for Istanbul (LTBA), with an intermediate stop at Manas Airport (UCFM) near Bishkek, the capital and largest city of Kyrgyzstan (Kyrgyz Republic). The cargo flight was operated on behalf of Turkish Airlines by ACT Airlines on Jan. 16, 2017. The planned time en route was 6 hr., 3 min. The crew conducted a preflight briefing beginning at 2130 Hong Kong time but did not depart until 0312, a delay of 2 hr., 2 min. from the scheduled departure. According to the accident report, the destination weather, although foggy, was “within limits to depart.” Two alternates, Astana (UACC) and Karaganda (UAKK), Kazakhstan, were filed.
The flight cruised at 34,000 ft. using the separation system of the People’s Republic of China and entered the Bishkek ATC Area Control Center at 0641 local time. (There is a 2-hr. time difference between Hong Kong and Bishkek.) Ten minutes later, the flight was cleared to descend to FL 220 (using the Kyrgyz Republic system) and shortly thereafter was advised that Manas Airport Runway 26 RVR was 1,300 ft. at the threshold and 1,000 ft. at midpoint and end, with vertical visibility of 130 ft.
The flight was handed off to Bishkek Approach Control at 0705 and cleared for the TOPKA 1 arrival and descent to FL 060 for an intended ILS approach to Runway 26. The controller reported the winds were calm, the visibility was 165 ft., the RVR was 1,000 ft., there was freezing fog and the vertical visibility was 160 ft. Asked by the controller if they wanted to continue the approach, the crew confirmed that they did. The airline’s operating manual allowed pilots to continue an approach up to 1,000 ft. above the runway threshold altitude regardless of provided RVR data.
At 0711:45, the flight was reminded of the transition level FL 060, given the QNH, 1023 hectopascals, and cleared for the ILS RWY 26. The approach controller added, “call me on localizer.” At 0714:05, the flight captured the localizer and 3 sec. later the glideslope mode armed. The pitch mode was flight level change and the selected altitude was set to 3,400 ft., the depicted glideslope altitude.
At 0715:13, the approach controller asked, “Turkish six four niner one, are you established?” and when the crew confirmed they were, handed them off to the tower. Bishkek Tower cleared the flight to land at 0715:38. The RVR had improved slightly to 1,300 ft. at the approach end, 1,065 ft. at the midpoint and 1,300 ft. at the runway end.
There was just one problem. The flight was too high to capture the normal glideslope. In fact, throughout the entire descent the airplane had been high on profile, and the crew knew it.
Kyrgyzstan is one of the most mountainous countries in the world; 94% of its lies above 1,000 meters (3,280 ft.), and peaks range up to 24,406 ft. MSL. Bishkek is in the far north and lies in one of the country’s few plains. The Manas Airport elevation is 2,090 ft. The depicted minimum safe altitude to the south of Manas is 13,000 ft. and 5,900 ft. to the east.
The TOPKA 1 arrival requires crossing 43 nm southeast of Manas (MNS) VOR/DME (RAXALT) at or above FL 170 and 16.2 DME southeast (TOPKA) at or above FL 060. These restrictions can be met if the crew makes prudent use of drag devices. But the flight remained high on profile throughout the descent, and the captain can be heard on the cockpit voice recorder (CVR) complaining about ATC. While still at FL 220, the captain says, “We are starting to be high.” Leaving FL 180 with clearance to cross TOPKA at FL 060, the captain says, “They left us high again.” The flight crossed TOPKA at 9,200 ft. and 270 kt. Crossing a waypoint (MNS 090/8) with a recommended altitude of 4,400 ft., the flight was at 6,500 ft. and had an airspeed of 220 kt.
At 0714:18, when the airplane was over the Manas VOR/DME 5.4 DME, it was supposed to be at the glideslope intercept altitude of 3,400 ft., but the crew were at 5,300 ft. When they intercepted the localizer, they continued descent to the glideslope intercept altitude, but they were already past the 3.2 DME where the glideslope began. They flew level at 3,400 ft. until 0.4 DME, just 1.15 nm from the runway threshold, before commencing their final descent. The Runway 26 threshold was 2,055 ft. MSL, and they were at 3,400 ft. just over a mile away.
The glidepath deviation indicator descended from its position at the top of the primary flight display, but the angle of the captured glideslope signal was not 3 deg.; it was 9 deg.
Six seconds after the (false) glideslope capture, the green “LAND 3” annunciation was recorded, indicating the autoland system was engaged in a triple redundant, fail-operative configuration, suitable for use in ICAO CAT III conditions. The captain called out, “Glideslope capture,” the first officer (F/O) responded, “Check. Four thousand four hundred,” and the captain said, “Land three.”
But then, 15 sec. after the glideslope signal capture, there was an autopilot caution, an amber line drawn through the glideslope mode annunciation, and the beginning of a “four beep” audio alert that lasted until the flare.
The autopilot continued to function. The pitch control channel maintained an inertially derived 3-deg. descent track, a descent designed to continue until either a valid glideslope signal reappeared, the crew disconnected the autopilot or the crew commenced a go-around. (This inertial path feature is common to Boeing 747-400/-8, 757, 767, 777, 787 and some 737 aircraft).
At 0716:18, the autoland mode changed from LAND 3 to LAND 2. The crew checked the altitude, which was 800 ft., and continued the approach. At a height of 300 ft., the EGPWS Mode 5 “glideslope” aural warning began to sound and continued until the flight passed 200 ft. At 0717:04, the 100-ft. aural warning sounded and the F/O called out, “Minimums.” At 0717:07, the captain commanded, “Negative, go around.”
At 0717:09, the autopilot FLARE mode engaged, then, at 58 ft., the go-around push button was pressed. Engine thrust began to increase, there was a control column pitch-up input, and vertical load increased to 1.4g. However, 3 sec. after the go-around button activation, the jumbo made ground contact.
The Investigation
The investigation was conducted by the Russian Interstate Aviation Committee (IAC) Air Accident Aviation Commission as the State of Occurrence by treaty agreement with Kyrgyzstan. Also participating was Turkey as the State of Registry and Operator and the U.S. as the State of Aircraft Design and Manufacture. The NTSB, FAA and Boeing represented the U.S. The IAC issued its final report this past February and provided a courtesy English translation.
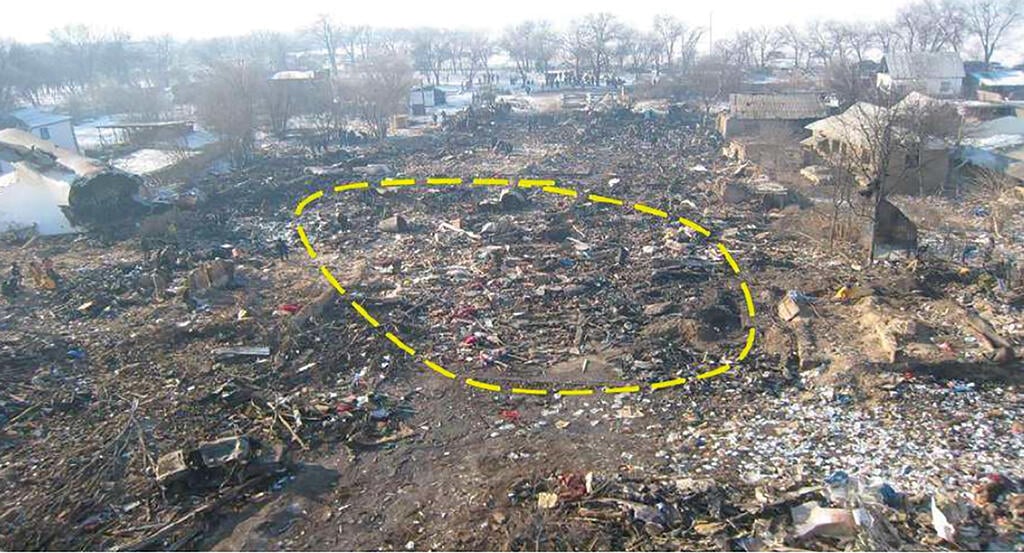
Examination of the accident site showed the 747’s right wing and engines impacted buildings about 525 ft. beyond the touchdown point, and the aircraft began to turn right while still moving forward. At 1,450 ft. beyond touchdown, the cockpit impacted a brick house and turned more than 90 deg. to the right. Parts of the left wing and empennage traveled about 100 ft. beyond the cockpit. Fuel spillage fed a fire that destroyed most of the aircraft.
The aircraft flight data recorder (FDR) and CVR were recovered, as was one of the three flight control computer (FCC) circuit boards. The FCC unit was sent to the NTSB and examined by Rockwell Collins, the manufacturer. The non-volatile memory data was successfully downloaded and used in the investigation. A recording of air traffic control transmissions was also obtained.

The captain, 59, had 10,808 hr. of flight time, including 820 hr. on the 747. His training records and medical certification were complete. He had a previous accident, a runway excursion and gear collapse at Bagram Airport while serving as an F/O in 2010.
The F/O, also 59, had 5,894 hr. total flight time and 1,758 hr. in the 747, and his training records and medical certification also were normal. Both pilots had been off duty in Hong Kong for 69 hr. before the flight, and both were on duty 11 hr., 47 min. at the time of the accident. The two had flown into Bishkek together the month before the accident. Both pilots were graduates of the Turkish Air Force Academy.
The airplane was manufactured in February 2003 and operated by Singapore Airlines from then until December 2015. Turkey’s ACT Airlines began operating the four-engine Boeing the following October. The airplane had logged 46,820 hr. and 8,308 cycles at the time of the accident. Its oldest engine was manufactured in 1991 and had over 90,000 total hours and had undergone three overhauls. Examination of maintenance records revealed no faults or areas of concern. A fuel sample taken from the left wing was found to be normal.
The freighter’s takeoff weight of 755,055 lb. and 213,055-lb. fuel weight were found to be in limits, as was the takeoff center of gravity of 23% of MAC. The landing weight of 614,649 lb. and 151-kt. Vref also were within limits and appropriate.
The weather at the Chuya lowland and Manas Airport on Jan. 15-16 was affected by a slow-moving cold front with a wide area of frontal fog and consecutive forecasts for fog, visibility 650 ft. and vertical visibility 100 ft. Investigators found the forecasts had been accurate and the meteorological equipment and support had been in compliance with requirements. The airfield lighting was checked and found to be functioning normally.
A Diamond DA-42 flying laboratory was used to fly the accident aircraft’s profile along the ILS and all parameters checked. The false glideslope was found, with an angle of about 8.8 deg., at 1.2 nm from the end of Runway 26 at 3,400 ft.
Analysis and Causes
The IAC’s lengthy analysis can be divided into four main areas:
(1) Conduct of the descent. The crew did not take the appropriate actions to get the airplane down to the required approach altitude. In particular, the descent between RAXALT and TOPKA, a distance of 27 nm, required the use of speed brakes and possibly lowering of the gear and possibly even the first notch of flaps in order to lose the depicted 12,000 ft. of altitude.
(2) Lack of assistance from ATC. Both the approach controller and the tower controller had radar with altitude capability, but the former was not required to notify the crew of their abnormal altitude and the latter had not been trained to use the radar for this purpose.
(3) The crew’s “psycho-emotional condition.” The captain displayed anxiety and even intemperance about the steep descent and the F/O’s efforts to calm him were not successful. The crew began to blame the controller for their own errors, stopped monitoring approach indications and narrowed their focus to only two objects — altitude and the autoland objective — all of which resulted in “tunnel effect.” In addition to violating their own airline flight operations manual guidance and mandatory callouts, they ignored the “AUTOPILOT” and “FMA FAULT 2” cautions, the audio beeper alert, the flight director pitch bars removed from the PFDs, the “G/S” indication with a crossed amber line, and the two “MASTER CAUTION” lights and audio alert. The crew was not psychologically prepared to go around.
(4) Boeing guidance and systems operation logic. The manufacturer’s flight crew operating manual (FCOM) and flight crew training manual (FCTM) do not provide a complete description of pitch mode failure or direct instructions for pilot actions in this case. There was some conflict between the FCTM and training manual guidance as to exactly when a go-around is required. Most significantly, the airplane’s system operation may not be in compliance with the FAA’s certification requirements.
The 14 CFR Part 25.1322 document “Flightcrew Alerting” requires red for warning alerts and amber or yellow for caution alerts. The green LAND 3 and LAND 2 annunciations are used for advisory purposes and informing the crew on safe operational conditions. The descent beyond the runway area in IFR ICAO II conditions was certainly not safe. The crew probably relied on the green advisory display. The IAC gave as a contrary example the red warning “APPROACH LOST” in the Sukhoi RRJ-95 when the glideslope signal is lost.
The FAA Advisory Circular on automatic landing systems that was in effect when the Boeing 747-400F was certified (AC 20-57A) set prescribed dispersion areas on the landing surface, and the accident landing was well outside those limits. The most recent update of that AC requires the probability of touchdown within that area of 1 x 10-6.
The false glideslope capture that took place and the followed inertial path with only an amber annunciation does not seem to be in full compliance with the established requirements.
The IAC found the cause of the accident was “the missing control of the crew over the aircraft position in relation to the glideslope during the automatic approach, conducted at night in the weather conditions, suitable for ICAO CAT II landing, and as a result, the measures to perform a go-around, not taken in due time with the aircraft, having a significant deviation from the established approach chart, which led to the controlled flight impact with terrain (CFIT) at the distance of ≈930 meters beyond the end of the active RWY.”
There were six contributing factors, paraphrased here:
- The flight crew’s poor briefing and descent planning.
- The flight crew’s poor execution of the descent, leaving them too high.
- The lack of the tower controller’s requirements to monitor aircraft deviations.
- The excessive psycho-emotional stress of the crewmembers.
- The flight crew’s lack of monitoring crossing reference points.
- The flight crew’s failure to verify altitude at the FAF/FAP and the lack of a depicted FAF on the Jeppesen chart.
Recommendations
The IAC wrote 13 recommendations, directed variously to airline managements, ATC personnel, airports, Boeing and the FAA. Several involved improved procedures and training at airlines, and ACT airlines has taken steps to address these concerns.
Four recommendations pertain to the airplane’s design and operational guidance. Paraphrased, they are:
Improve glideslope capture logic and false glideslope warning.
Change the inertial glideslope descent logic.
Provide a better description of the inertial path flight mode.
Eliminate guidance discrepancies for “autopilot caution.”
In its earlier preliminary report, the IAC had urged the FAA to reevaluate the Boeing 747’s compliance with certification requirements. The FAA replied that they believed the aircraft met all requirements and did not envisage any reasons for changing the logic of the automatic flight system.
While I have great respect for the millions of successful ILS and autoland approaches the Boeing fleet has made over the years, I think this accident points up a discrepancy in the Boeing approach display that should be addressed. The color green has universally meant “normal” in aircraft displays. In addition, green has a broader meaning in everyday life. When you see a green traffic light, it means one thing: Go! When a crew is missing their marks, green is not the color they should be seeing when danger lurks. The color green just has too much power for that.
Related Content




