
Delayed action with bad consequences.
What follows are two landings on shorter, wintry runways with unfortunate outcomes, both caused in part by tardy procedures. And both could have been avoided altogether by simply landing elsewhere.
Automatic terminal information service (ATIS) “Bravo” was current on Oct. 27, 2016, when the first officer (F/O), who was the pilot flying the chartered Boeing 737-7, began to brief the instrument landing system approach for Runway 22 at New York’s LaGuardia Airport (KLGA). The broadcast indicated visibility, 3 mi. in rain; ceiling, 1,500 ft. broken, overcast at 2,200 ft.; wind from 130 deg. at 9 kt.; and that braking action advisories were in effect. (The airplane’s automatic speed brake module had been deactivated two days earlier and deferred in accordance with the operator’s minimum equipment list, which was appropriate.)
In post-flight interviews, the pilot stated that the flight had been completely normal from departure in Kansas until final approach, when it encountered moderate to heavy rain.
The flight crew completed the approach briefing after descending through 18,000 ft. MSL and completed the landing checklist when the airplane was near the final approach fix. The airplane was configured for landing with the autobrake set to 3 (highest setting before max) and the flaps set to 30 deg. ATIS information “Charlie” was current at that time and indicated visibility, 3 mi. in rain; ceiling, 900 ft. broken, overcast at 1,500 ft.; and wind from 120 deg. at 9 kt. Previous flights described breaking out 2 to 300 ft. above the ground with light and occasional moderate turbulence.
Flight Parameters
To be stabilized, all of the following conditions must be achieved prior to, or upon, reaching stabilization height:
- The aircraft is on the correct lateral flight plan.
- The aircraft is in the desired landing configuration.
- The thrust is stabilized above idle, to maintain the target speed on the desired glidepath.
- There is no excessive flight parameter deviation.
If the aircraft is not stabilized on the approach path in landing configuration, at 1,000 ft. (above TDZE) in instrument conditions, or at 500 ft. (above TDZE) in visual conditions, a go-around must be initiated. Or if an aircraft is not stabilized as described in stabilized approach or flight parameters, a go-around should be initiated.
Flight data recorder (FDR) information and post-incident flight crew statements indicate that the airplane was stabilized on the approach in accordance with the operator’s procedures until the flare. The airplane crossed the runway threshold at 66 ft. radio altitude at a descent rate of 750 ft. per minute. When the airplane had traveled about 2,500 ft. beyond the runway threshold, its descent rate decreased to near zero, and it floated during the flare. Its pitch attitude started to increase in the flare from 2.8 deg. at a radio altitude of about 38 ft., which is high compared to the 20 ft. recommended by the Boeing 737 Flight Crew Training Manual.
Further, the F/O didn’t fully reduce the throttles to idle until about 16 sec. after the flare was initiated and after the airplane had touched down. The initiation of the flare at a relatively high altitude above the runway and the significant delay in the reduction of thrust resulted in the airplane floating down the runway, prompting the captain to tell the F/O to get the airplane on the ground, stating first “down” and then about 3 sec. later, “down, down, down, down. You’re 3,000 ft. remaining.”

The airplane eventually touched down 4,242 ft. beyond the runway threshold. According to the operator’s procedures, the touchdown zone for Runway 22 was the first third of the 7,001-ft.-long runway beginning at the threshold, or 2,334 ft. The airplane’s groundspeed at touchdown was 130 kt.
Two of the witnesses, a limo driver and a police officer, both stated that they thought the airplane was moving much faster than other landings they had observed both that night and other nights with the same airplane at the same facility.
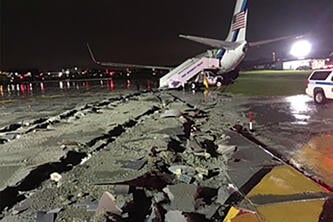
The captain manually deployed the speed brakes about 5 sec. after touchdown and after the airplane had traveled about 1,250 ft. farther down the runway. The company’s “Speed Brake Not Armed” procedure calls for immediate deployment after touchdown. Maximum reverse thrust was commanded about 3.5 sec. after the speed brakes were deployed, and, with fully extended speed brakes and maximum wheel brakes (which were applied at main gear touchdown) the airplane achieved increasingly effective deceleration. Its groundspeed was about 35 kt. when it entered the EMAS (engineered materials arrestor system) overrun area. With the effective deceleration provided by the fully extended speed brakes, maximum wheel brakes and reverse thrust, the flight crew would have been able to safely stop the airplane if it had touched down within the touchdown zone.
The captain later stated he had considered calling for a go-around before touchdown, but the “moment had slipped past and it was too late.” He said that “there was little time to verbalize it” and that he instructed the F/O to get the airplane on the ground rather than call for a go-around. He reported that, in hindsight, he should have called for a go-around the moment that he recognized the airplane was floating in the flare. For his part, the F/O said he did not consider a go-around because he did not think that the situation was abnormal at that time.
Following the incident, the operator incorporated go-around training scenarios in which flight crews must decide to go around rather than being instructed to do so. It also added a training module emphasizing that “if touchdown is predicted to be outside of the [touchdown zone], go around” and intended to require a go-around if landing outside of the touchdown zone were predicted. The operator also intended to incorporate go-around planning into the approach briefing.
Analysis of the FDR showed that 1 sec. after touchdown the nosegear became airborne again for 2.25 sec. This further added to the stopping distance for the flight.
Under the existing conditions, according to the final report, the captain’s manual deployment of the speed brakes was not timely. NTSB analysis of FDR data for previous landings in the incident airplane determined an average of 0.5 sec. for manual deployment of the speed brakes. Using the same touchdown point as in the incident, post-incident simulations suggest that, if the speed brakes had been deployed 1 sec. after touchdown followed by maximum reverse thrust commanded within 2 sec., the airplane would have remained on the runway surface.
Further, the airline had a procedure in which the captain was to make callouts that state that he had control of the airplane when he assumed control on the ground. Contrary to those procedures, the incident captain did not make those callouts. Further, he took control of the airplane with the copilot still considering himself to be in control and commanded directional control inputs that countered those by the F/O. The captain later reported that he had forgotten that an EMAS was installed at the end of Runway 22 and attempted to avoid the road beyond the runway’s end by applying right rudder because he thought it would be better to veer to the right. However, the F/O officer applied left rudder to maintain alignment with the runway centerline and to counter the airplane pulling “really hard” to the right because of the captain’s inputs. The breakdown of crew resource management during the landing roll and the captain’s failure to call for a go-around demonstrated his lack of command authority, which contributed to the incident.
The crew felt the flight had proceeded normally until the overrun and neither felt uncomfortable with the other’s performance. The company was building a new safety management system (SMS) and had not yet reached the deadline for the completion of the administration of the plan. And a tool “designed to help with safety risk assessment, assurance and risk management” was still under development.
The NTSB determined the probable causes of this incident to be the F/O’s failure to attain the proper touchdown point and the flight crew’s failure to call for a go-around, which resulted in the airplane landing more than halfway down the runway.
Contributing to the incident were the F/O’s initiation of the landing flare at a relatively high altitude and his delay in reducing the throttles to idle, the captain’s delay in manually deploying the speed brakes after touchdown, the captain’s lack of command authority, and a lack of robust training provided by the operator to support the flight crew’s decision-making concerning when to call for a go-around.
Eleven years earlier, on Dec. 8, 2005, about 1914 Central Standard Time, another Boeing 737-7 ran off the departure end of Runway 31C after landing at Chicago Midway International Airport (KMDW). The airplane rolled through a blast fence and an airport perimeter fence, and then onto an adjacent roadway where it struck an automobile before coming to a stop.
The collision killed a child in the car and seriously injured another person in it; three other persons in the automobile received minor injuries. Eighteen of the 103 people in the airplane received minor injuries, and the airplane was substantially damaged.
The flight had departed nearly 2 hr. late, due to a weather-related gate hold, from Baltimore/Washington International Thurgood Marshall Airport (KBWI) in Maryland, about 1758 Eastern Standard Time. Instrument meteorological conditions prevailed at the time of the accident flight, which operated on an instrument flight rules flight plan.
While en route, the pilots read the ATIS information several times and input data into the onboard performance computer. According to investigators, the flight crew input all possible wind and runway condition scenarios and set parameters for which they would not attempt the approach. Through these exercises they determined that they would stop 560 ft. from the end of the runway with “fair” conditions and 30 ft. from the end of the runway if conditions were “poor.” The performance computer could only take one condition, “poor” or “fair” at a time.
There was discussion in the cockpit about using the autobrake system, as this was a relatively new procedure with the airline. The captain was initially hesitant, but eventually the F/O convinced him to use them. The captain mentioned that he had seen them work in the simulator and in a previous trainer mission and was very impressed with their operation.
Arriving in the Chicago area they were initially given a hold while the runway was being plowed.
According to the cockpit voice recorder (CVR) transcript, when the pilots contacted the KMDW air traffic control tower at 1909:53.7, controllers advised them to “continue for 31C the winds zero nine zero at nine, braking action reported good for the first half, poor for the second half.” About 1912:28, the F/O received a landing clearance.
FDR information indicated that the airplane was aligned on the runway centerline as it touched down at an airspeed of about 124 kt. The speed brakes deployed and the brake pressure increased within about 1 sec. Both pilots described the touchdown as “firm.” That was as intended as the captain stated he did not want to follow HGS flare guidance as he felt it would land them too far down the runway.
The captain stated that he tried to deploy the thrust reversers immediately after touchdown but had difficulty moving the thrust reverser levers to the reverse thrust position. He further stated that he felt the anti-skid system cycle after the airplane touched down but then felt it stop cycling, and that the airplane seemed to accelerate. He said that he subsequently applied the wheel brakes manually but made no further effort to activate the thrust reversers. He told investigators that he believed that the use of the autobrake system distracted his attention from the thrust reversers after his initial attempt to deploy them.
The F/O said that, when he sensed a decrease in the airplane’s deceleration during the landing sequence, he exclaimed, “brakes, brakes, brakes,” and manually applied the brakes. He stated that he then looked at the throttle console and saw that the thrust reverse levers were still in the stowed position. The F/O moved the captain’s hand away from the thrust reverser levers and, about 15 sec. after touchdown, initiated deployment of the thrust reversers to the maximum reverse setting. FDR evidence confirmed the systems functions described by the pilots and indicated that full thrust reverser deployment occurred about 18 sec. after touchdown.
The F/O stated that, after the airplane came to a rest, he performed the emergency evacuation checklist while the captain checked on the passengers in the cabin. The passengers evacuated through the forward left and the right rear cabin doors.
Pilot and forward flight attendant debriefings indicate a very orderly evacuation was performed with the captain and flight attendant standing near the forward left exit door and not allowing passengers to carry luggage off the airplane. The copilot was stationed on the ground and a dead-heading pilot reported to the captain when the airplane was empty. The captain returned to the cockpit one last time to ensure it was secure.
Among the findings by the NTSB:
(1) The company failed to provide its pilots with clear and consistent guidance and training regarding company policies and procedures related to arrival landing distance calculations.
(2) Programming and design of the aircraft’s onboard performance computer was inadequate since it did not present inherent assumptions in the program critical to pilot decision making.
(3) New autobrake procedures were implemented without a familiarization period.
(4) There was a failure to include a margin of safety in the arrival assessment to account for operational uncertainties.
Also contributing to the accident was the pilots’ failure to divert to another airport given reports that included poor braking action and a tailwind component greater than 5 kt. And contributing to the severity of the accident was the absence of an EMAS, which was needed because of the limited runway safety area beyond the departure end of Runway 31C.

Related Content





Comments